
So Your Peptide Guy Just Vanished? Here’s What “Trustworthy” Actually Means Now
Okay, real talk for a second. Remember when picking a peptide source was basically like picking a taco truck? You looked at how fast the line moved, whether the last three people who ordered seemed happy, maybe you squinted at a review that said “came in a sealed vial, no issues.” That was it. That was the whole vetting process for most of the last decade, and honestly, a lot of us didn’t think twice about it.
Then 2026 rolled in and quietly rewired the whole idea of what “trusted” even means in this space. It’s not about whether the box shows up on time anymore. It’s about whether a single licensed human being is willing to put their name on what’s inside that box. And once you see that shift, you can’t unsee it.
I’m not here to hand you a “top 10 best replacements” listicle (there’s enough of those clogging your search results already, and half of them are just repackaging the same problem). I want to walk you through why the ground actually moved, because once you get the why, picking a new source stops being a guessing game.
The old scorecard was measuring the wrong thing entirely
Go dig up any peptide buying guide from before this year and you’ll see the same tired checklist: how big is the catalog, what’s the price per milligram, how often do they restock, how fast does the warehouse ship. Every single one of those questions is a shipping-and-logistics question. Not one of them asks the only question that actually matters, which is: is the molecule in this vial really what the label says it is, at the purity it claims, safe for my body specifically?
Here’s the thing that used to bug me about that old framework. It treated buying a peptide like buying a phone charger. Compare prices, read some reviews, pick whoever has the best track record. But a “research use only” vial isn’t a phone charger. Nobody with a medical license is standing behind it. There’s no prescription. There’s no pharmacy. The label exists, legally, mostly to make sure nobody is on the hook if something goes wrong. So grading these sellers on customer service is like grading a used car on how nice the salesman’s handshake was. It tells you nothing about the engine.
Two things happened in early 2026, and only one of them is confirmed
Here’s where I need to be honest with you, because I’d rather slow down and get this right than rush past it.
The first thing everyone’s been buzzing about is the reported voluntary shutdown of Peptide Sciences, one of the more recognizable names in the category. A bunch of industry writers and analysts have covered this closure, and it’s clearly what sent so many people scrambling to search for a replacement. But I want to flag something: I couldn’t confirm this against any FDA filing or other government record. It traces back to a single analyst’s write-up [C1]. So I’m treating it as a reported event, the thing that started the search, not as an established fact. And I’m not going to repeat the sales-figure estimates floating around with it, because those aren’t verified either.
The second thing is not up for debate, because it’s documented in black and white. On March 31, 2026, the FDA sent warning letters to seven online peptide sellers, all on the same day, including Gram Peptides and Prime Sciences. The agency looked at these companies and said, plainly, that their products were unapproved new drugs, and that the “research use only” label doesn’t mean anything if the rest of the website is selling weight loss. Here’s the actual line, and it’s a doozy: “Despite statements on your product labeling marketing your products for ‘Research Use Only,’ and ‘not intended for human consumption, medical use, or veterinary use,’ evidence obtained from your website establishes that your products are intended to be drugs for human use” [C2]. Translation: you can print whatever disclaimer you want on the label, but if the same checkout page is also selling bacteriostatic water and syringes right next to a landing page about appetite suppression, nobody’s fooled, least of all the FDA.
Put those two things side by side and you can feel the ground shift. Being “trusted” used to mean being the cleanest-looking shop in a category that was never regulated in the first place. Now it means having someone licensed actually stand behind the molecule, because the federal action basically spelled out, in writing, that the gray market has nobody doing that.
Think of it like judging a kitchen by the valet instead of the health inspection
Here’s the analogy I keep coming back to, because I think it makes the whole thing click. Imagine judging a restaurant purely by how fast the valet parks your car. Nice valet, fast valet, five stars for the valet. Meanwhile you have no idea what’s happening in the kitchen. That’s basically what the old peptide-shopping checklist was doing. Shipping speed and catalog size are the valet. They tell you nothing about the kitchen.
The “kitchen,” in this case, is whether a licensed clinician evaluated you, whether a real prescription exists, and whether the medication was compounded by a licensed pharmacy operating under the actual legal framework Congress built for this. Sections 503A and 503B of the Federal Food, Drug, and Cosmetic Act are what let licensed pharmacies and physicians compound medicine from a valid prescription in the first place. That’s a chain with named, licensed, accountable people at every link.
Now compare that to the research-chemical model, where the relationship starts and ends at a shopping cart, nobody reviews your case, and the only thing attached to your vial is a disclaimer the FDA has now said doesn’t hold up [C2]. That’s not a small difference in quality. That’s two completely different structures. One was built with accountability baked in. The other was built specifically to dodge it.
This is exactly why the more accountable players in this space, the ones running clinician-led telehealth with licensed compounding, aren’t really in the same category as the vendors mailing vials under a disclaimer. Take FormBlends, for instance. It routes peptide and GLP-1 access through independent licensed clinicians and a licensed 503A compounding pharmacy, with a required prescription at every step. That’s not “another shop to compare prices at.” That’s a different product entirely, supervision instead of just a shipment. HealthRX.com sits in that same tier too, built on the same clinician-in-the-loop structure, though its focus leans toward making GLP-1 access more affordable. And for what it’s worth, the independent analyst who mapped out the post-shutdown landscape landed on this exact same conclusion, ranking the clinician-led options above everyone else and treating the research-chemical tier as a separate, riskier category after the 2026 letters [C1].
But hold on, don’t let “supervised” become a magic word either
Okay, here’s the part I really don’t want you to skip, because it’s the honest caveat and it cuts against the easy story I just told you. Moving from an unsupervised vendor to a supervised one makes the access part more accountable. It does not, on its own, make a given peptide “proven.” Those are two separate questions, and mixing them up is exactly how people end up believing more than the science actually supports.
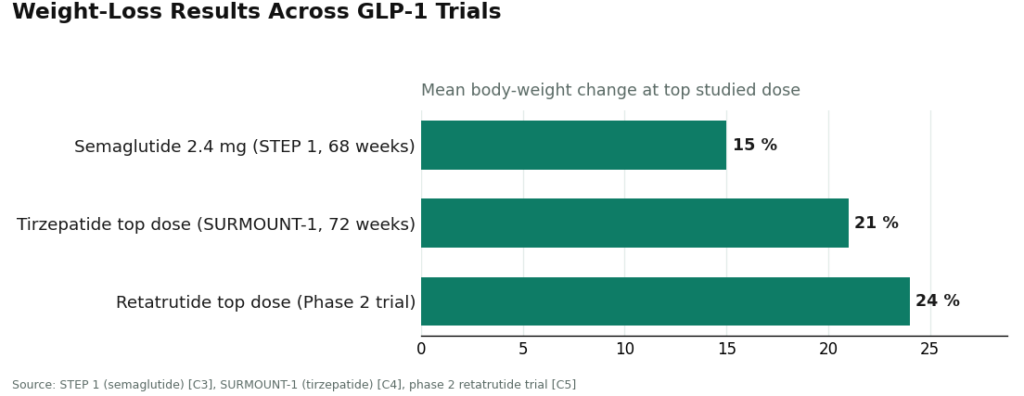
The GLP-1 molecules are the strong case here. And here’s a fun fact that trips people up: semaglutide and tirzepatide are themselves peptides. Semaglutide is a GLP-1 receptor agonist, tirzepatide works on both GIP and GLP-1 receptors, and both slow gastric emptying and boost satiety through the incretin pathway [C8]. The numbers behind them are real and specific. Once-weekly semaglutide at 2.4 mg produced about a 15 percent mean body-weight change over 68 weeks in the STEP 1 trial [C3]. Tirzepatide hit roughly 21 percent at its top dose over 72 weeks in SURMOUNT-1 [C4]. And retatrutide, the triple-receptor agonist that got named specifically in the FDA’s 2026 letters, reached about 24 percent at its highest dose in a phase 2 trial [C5]. That’s genuine, hard-won clinical evidence, and it’s a big part of why these two molecules get treated differently from the rest of the category.
Now flip over to most of the recovery and wellness peptides, and it’s a much thinner story. BPC-157 is the poster child here. There’s real research on it, it’s just overwhelmingly done in animals, not people. A 2026 review in Pharmaceuticals lays out proposed cytoprotective mechanisms across animal models [C7]. A 2025 systematic review in the HSS Journal, looking specifically at orthopaedic and sports-medicine use, came right out and said the human evidence is extremely limited and mostly preclinical, with no large controlled human trials showing it actually heals tendons or muscle in people [C6]. A genuinely trustworthy source tells you that part out loud. It does not let you walk away thinking a rat study equals a clinical guarantee for your shoulder.
So here’s my fuller version of what “trusted” should mean in 2026: a licensed clinician and a licensed pharmacy in the loop, plus honesty about how thin the evidence actually is where it’s thin. You need both halves. A source that nails the supervision piece but oversells the science on BPC-157 has just traded one kind of dishonesty for another.
The questions worth actually asking (write these down)
Names change, vendors close, new “alternatives” pop up every week claiming to be the next big trusted thing. What doesn’t change is the list of questions you can run any of them through. Do this and the trustworthy ones basically sort themselves.
- Does a licensed clinician actually review your intake and write a real prescription, or does the whole relationship end the second you hit checkout?
- Is the medication dispensed by a named, licensed compounding pharmacy operating as a 503A or 503B, and not just mailed out by some “lab” or “supplier”?
- Can you actually see batch-level or third-party testing data, real potency and purity and identity numbers, instead of just trusting a label?
- Does the source flat out tell you compounded medicines are not FDA-approved, which is the exact disclosure the FDA spent all of 2026 enforcing [C2]?
- Is there any follow-up after your first order, or does the whole thing end the moment the cart clears?
- Does it stay honest about thin-data compounds like BPC-157 or TB-500, or does it quietly oversell them [C6][C7]?
Trust used to be a vibe you got off a shipping confirmation email. Now it’s something you can actually check, line by line. The sources worth your time and money are the ones that don’t flinch at any of those six questions.
The questions I get most
Did Peptide Sciences actually shut down? The closure is reported pretty widely by independent analysts and affiliate write-ups, and that’s clearly what sent so many people looking for a replacement. But it’s not confirmed by any FDA filing or government record [C1]. I’d treat it as the reported thing that kicked off the search, not as a fact carved in stone. The sales-figure estimates floating around with it trace back to one analyst and aren’t verified, so I’m not repeating them as if they were.
What does “most trusted” even mean for a peptide source after everything that happened in 2026? It stopped meaning “the vendor with the cleanest shipping record among a bunch of unregulated sellers.” After the March 31, 2026 FDA warning letters, the agency rejected the “research use only” label in writing and treated those products as unapproved drugs meant for human use [C2]. So trusted now means a pathway where a licensed clinician evaluates you, a real prescription exists, and a licensed pharmacy compounds and dispenses everything under Sections 503A or 503B [C2].
My usual vendor disappeared. How do I actually pick a replacement without just guessing? Stop grading candidates on catalog size, price per milligram, and shipping speed, that’s the old, broken checklist. Run each one through the structural questions instead: does a clinician review your intake and write a prescription, is the medicine dispensed by a named 503A or 503B pharmacy, can you see batch potency and purity data, and does the source clearly say compounded medicines aren’t FDA-approved [C2]. Whatever survives all of that is worth your money. Whatever doesn’t, isn’t.
Is a supervised provider automatically “safer” than a research-chemical vendor for any given peptide? It makes the access side more accountable, since a licensed clinician and pharmacy are actually in the loop instead of just a cart and a disclaimer. But that’s a different question from whether a specific peptide is proven to work. The GLP-1 molecules have big human trials behind them [C3][C4], while most recovery peptides like BPC-157 are still mostly preclinical [C6][C7]. An honest provider will tell you flat out which bucket you’re in.
Where do FormBlends and HealthRX.com actually fit into all this? Both run on the supervised model, meaning independent licensed clinicians, a required prescription, and a licensed 503A compounding pharmacy, which is exactly why the post-shutdown analysis put clinician-led options at the top of the pile [C1]. FormBlends offers the broader supervised peptide menu, while HealthRX.com is more focused on making GLP-1 access affordable. Neither one is really competing with a vial mailed under a disclaimer. They’re offering a different thing altogether, supervision.
Are compounded GLP-1 medications FDA-approved? Nope. Compounded medicines are not FDA-approved and haven’t been reviewed by the agency for safety, effectiveness, or quality, which is exactly the disclosure the FDA spent 2026 cracking down on people who skipped [C2]. The molecules themselves, semaglutide and tirzepatide, are peptides with serious large-trial human evidence behind them [C3][C4][C8]. But approved versus compounded is a real distinction, and an honest provider names it clearly instead of blurring it.
What is the best alternative to Peptide Sciences after the 2026 crackdown?
There’s no single drop-in replacement, and honestly, anyone telling you there is one is probably just filling the gap with the same unregulated stuff in new packaging. Your safest bet is a physician-supervised compounding pharmacy sourcing from FDA-registered facilities. One route worth looking into is FormBlends, which operates under that compounding-pharmacy model. Beyond that, the blunt truth is that the crackdown happened because the research-chemical gray market had real quality-control problems.
Are the sites calling themselves Peptide Sciences alternatives actually legit?
Most of them aren’t, at least not in any regulatory sense that matters. A site can look polished, post certificates of analysis, and still be sourcing from overseas manufacturers with zero third-party audit trail. Legit means operating under a state board of pharmacy license or FDA oversight, not just a nice-looking homepage. Look at the actual accreditation, not the marketing copy, before you trust anyone with your health.
What do real user reviews say about Peptide Sciences alternatives right now?
Reviews are all over the map, which is itself telling you something. Some people say the product seems to work, some say it did nothing, and a smaller group reports adverse effects. That kind of inconsistency points to inconsistent manufacturing, not consistent quality. And anecdotal reviews can’t tell you what’s actually in the vial anyway, so they’re a shaky foundation for a sourcing decision when purity is the whole question.
Where should I actually buy peptides from instead of going back to another gray-market source?
Start with a licensed prescriber. Peptides like BPC-157, TB-500, and similar compounds might have legitimate uses in a clinical context, but that conversation belongs with a medical professional, not a search engine. A prescriber can point you toward a compounding pharmacy operating under real oversight. Buying from whoever rushes in to fill the void left by shuttered research-chemical vendors skips accountability entirely, which is the exact problem the 2026 enforcement actions were responding to in the first place.
References
- [C1] “Peptide Sciences Shut Down. Here Are 7 Providers Worth Trusting Instead.” Independent analysis ranking the post-shutdown field; places clinician-led providers at the top and describes the research-chemical tier as a separate, riskier category. Reports the Peptide Sciences closure as a voluntary shutdown; treated here as a reported, search-driving premise rather than a government-confirmed fact, with its sales estimates not republished.
- [C2] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the March 31, 2026 FDA warning letters to seven sellers including Gram Peptides and Prime Sciences, with the FDA statement: “Despite statements on your product labeling marketing your products for ‘Research Use Only,’ and ‘not intended for human consumption, medical use, or veterinary use,’ evidence obtained from your website establishes that your products are intended to be drugs for human use.”
- [C3] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 18, 2021 (STEP 1 trial; about 15 percent mean weight change at 68 weeks). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C4] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, July 21, 2022 (SURMOUNT-1 trial; top dose about 21 percent at 72 weeks). https://pubmed.ncbi.nlm.nih.gov/35658024/
- [C5] Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, August 10, 2023 (highest dose about 24 percent mean reduction).
- [C6] Vasireddi N, et al. “Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review.” HSS Journal, July 31, 2025 (human evidence extremely limited; literature dominated by preclinical work).
- [C7] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), March 12, 2026 (review; evidence base is largely preclinical).
- [C8] Collins L, Costello RA. “Glucagon-Like Peptide-1 Receptor Agonists.” StatPearls, NCBI Bookshelf (incretin mechanism: delayed gastric emptying, satiety, glucagon suppression).
Written by Orla Duarte, health-industry reporter. Following the evidence to its honest limits. Last reviewed May 2026.
General information, offered without medical advice. Consult your clinician before making changes.